Make every note meet clinical, quality, and revenue cycle requirements.
Working in real time across the whole stay, Sayvant captures the reasoning and complexity of care, checks it against clinical guidelines and the standard of care, and produces notes that are complete, evidence-aligned, and valued for the care delivered.










The chart is where clinician pressure and financial pressure meet every day.
The note has to defend decisions that have already been made, while satisfying three readers at once. None reads the chart the way the others do.
Clinical
Documentation steals time from patient care, and incomplete notes leave the next clinician without the context to continue it.
Quality and risk
Gaps in documented reasoning make delivered care look subpar in retrospect, when it comes up in peer review or malpractice defense.
Financial
Cases are under-reimbursed because charts don't support the codes the care justifies, and poor defensibility drives denials and rework.
Today's approaches only address one piece each.
One documentation quality platform for every chart.
Sayvant satisfies all three readers at once, on every chart. It captures the reasoning as the clinician works, checks it against the standard of care, and makes sure the record reflects the full complexity of what was done before sign off.
The thinking behind the care
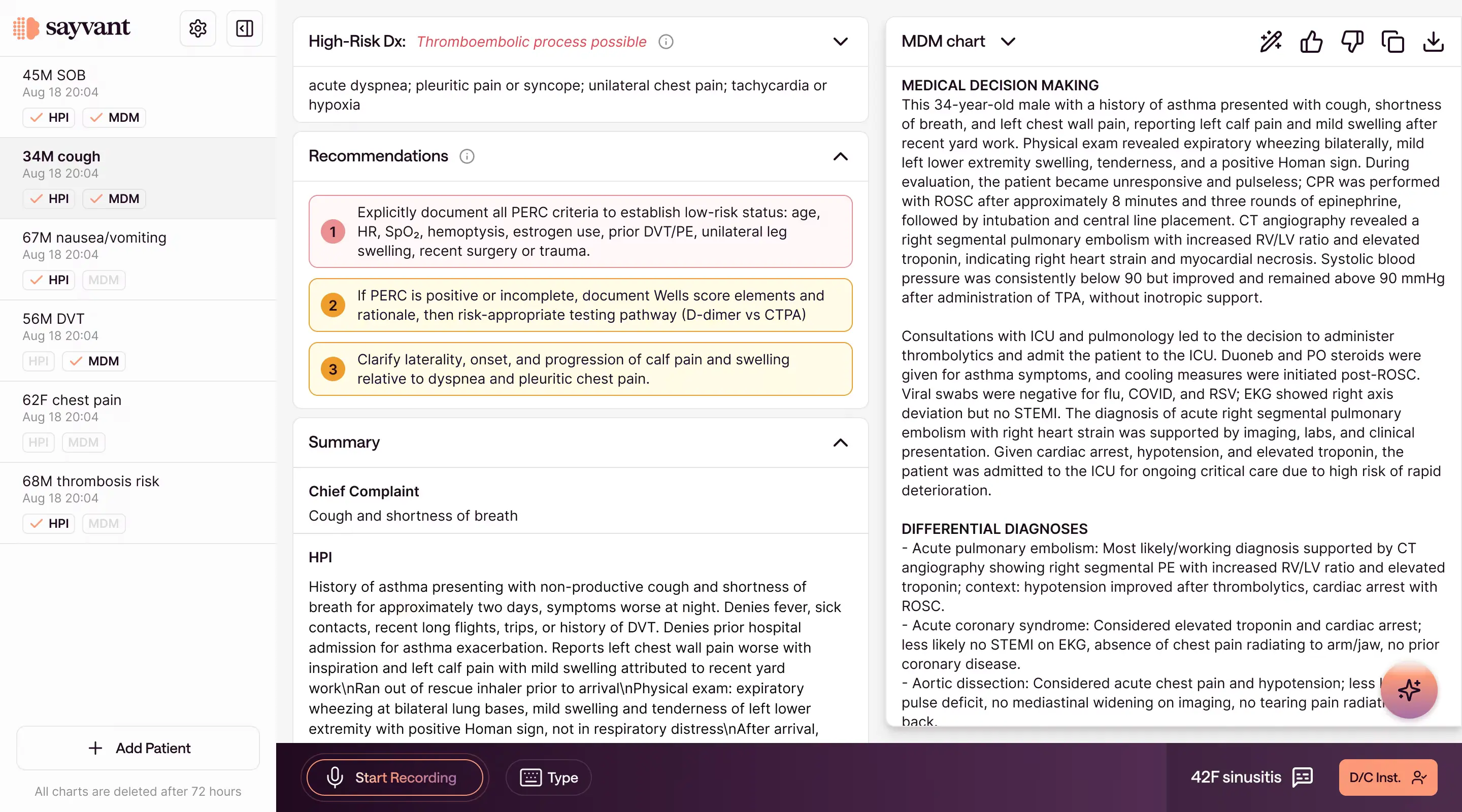
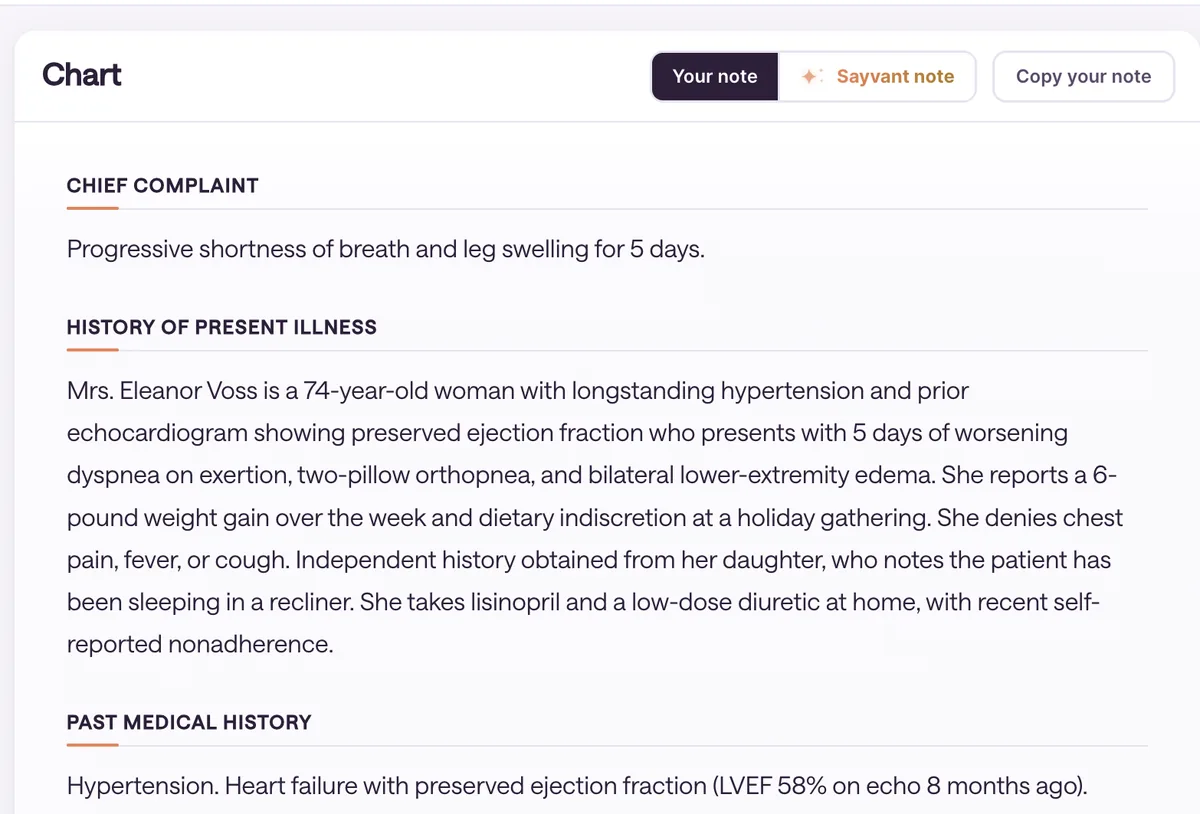
Sayvant generates notes that reflect the clinician's actual reasoning and the complexity of the visit, across the whole stay from ED through discharge.
- Gathers the case from ambient listening, dictation, and EMR data
- Surfaces high-risk differential diagnoses for consideration
- Generates full H&Ps, MDMs, and A&Ps
Aligned with the standard of care
Sayvant checks each diagnosis and plan against clinical evidence and guideline definitions before sign-off, and flags gaps and improvement opportunities.
- Surfaces next steps and best practices from trusted guidelines like ACEP and BMJ
- Flags missing pertinent information, from time stamps to interpretations
- Reviews medical necessity and clinical appropriateness at admission
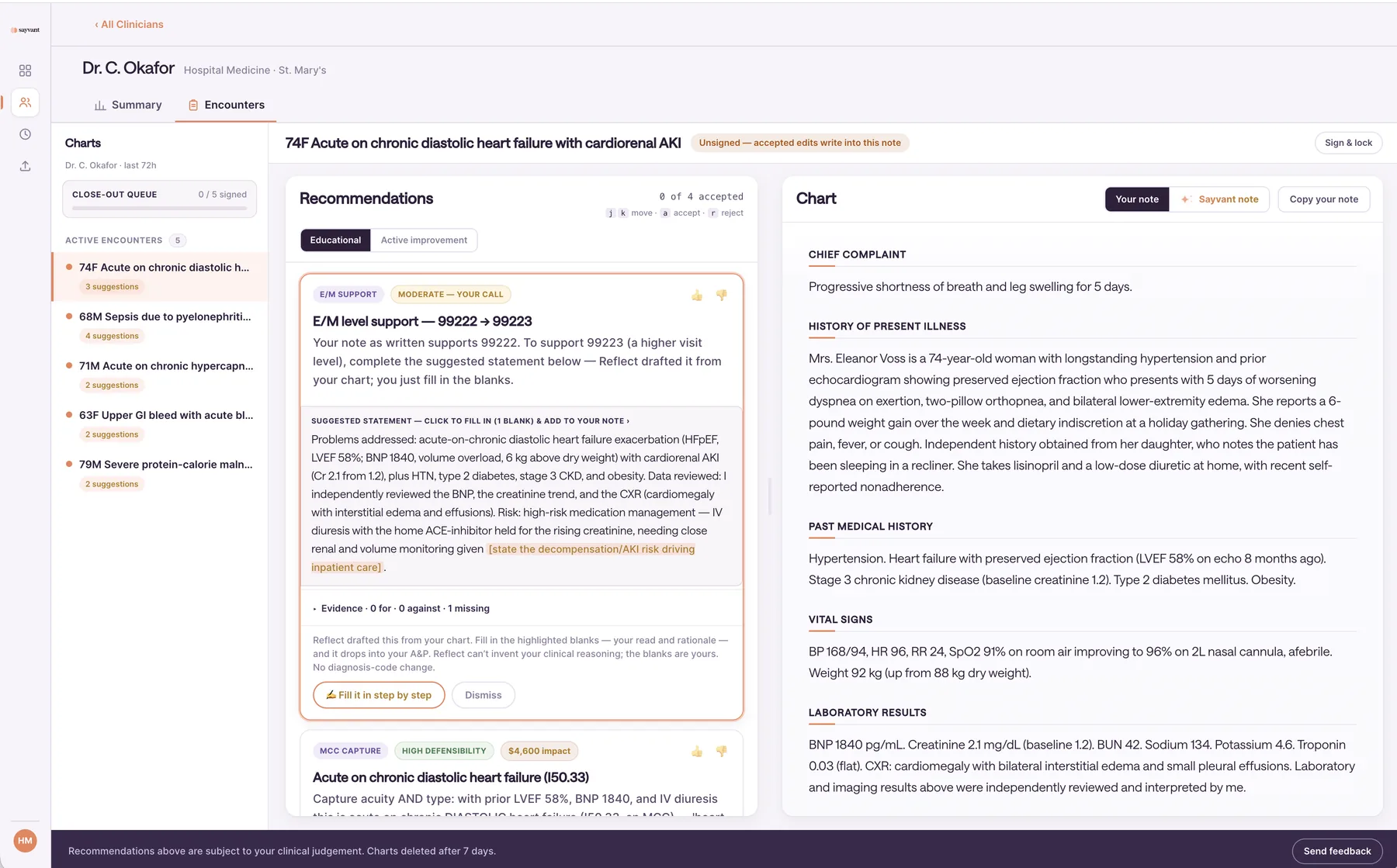
Valued for the care delivered
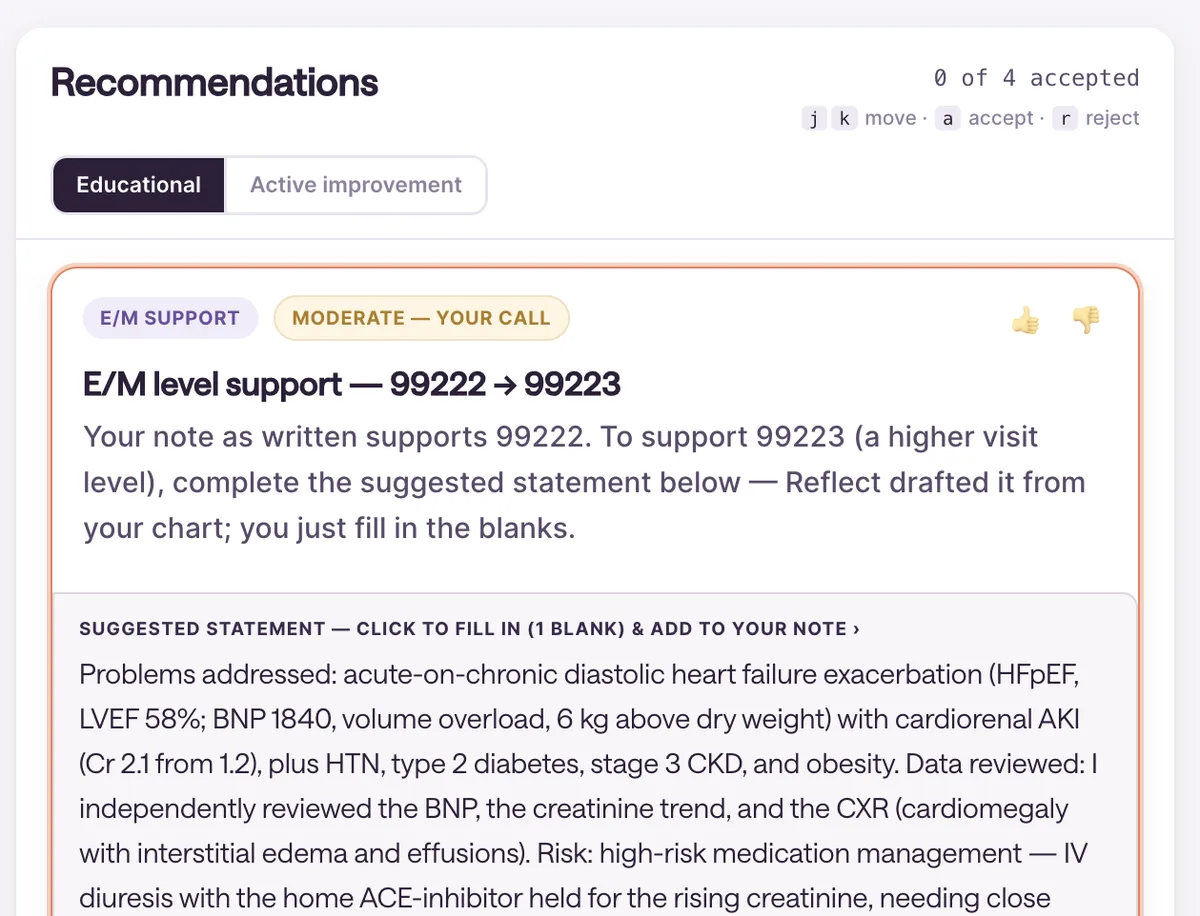
Sayvant documents the care delivered in line with reimbursement guidelines: medical necessity, diagnosis specificity, and complexity of care.
- Captures CPT codes for professional fees, including E/M level, critical care, and ACP
- Suggests DRG bundles based on the chart and clinical plan
- Reviews medical necessity against system guidelines

The only per-note quality score in acute care.
Underneath the platform is a physician‑validated scoring system built with an advisory panel of 10 board‑certified emergency physicians.
It grades every note on completeness, clinical quality, and financial defensibility, giving medical directors one number to hold the group to and a clear view of where documentation varies clinician to clinician.
Learn more →