Great care deserves a chart that proves it.
Sayvant works across the whole stay to capture clinical reasoning, assess documentation against quality guidelines, and ensure every signed note is valued appropriately.











The chart is where clinical reality
and financial pressure collide.
Every note is read by oncoming clinicians, quality leadership, CDI/UM, RCM, and payers.
Clinical
MDsCharting steals time from care, and rushed notes transmit an incomplete picture to the oncoming clinician.
Quality and Risk
CMOReviewers see the chart, not the patient. Undocumented reasoning results in perceived gaps in care.
Financial
CDI + UM + RCMPayers deny codes the chart can't defend. Revenue earned at the bedside is lost in the record.
Sayvant improves note quality.
Chief Complaint
Cough and shortness of breath
HPI
History of asthma presenting with non-productive cough and shortness of breath for approximately two days, symptoms worse at night. Denies fever, sick contacts, recent long flights, trips, or history of DVT. Denies prior hospital admission for asthma exacerbation. Reports left chest wall pain worse with inspiration and left calf pain with mild swelling attributed to recent yard work.
The thinking behind the care
Chief Complaint
Cough and shortness of breath
HPI
History of asthma presenting with non-productive cough and shortness of breath for approximately two days, symptoms worse at night. Denies fever, sick contacts, recent long flights, trips, or history of DVT. Denies prior hospital admission for asthma exacerbation. Reports left chest wall pain worse with inspiration and left calf pain with mild swelling attributed to recent yard work.
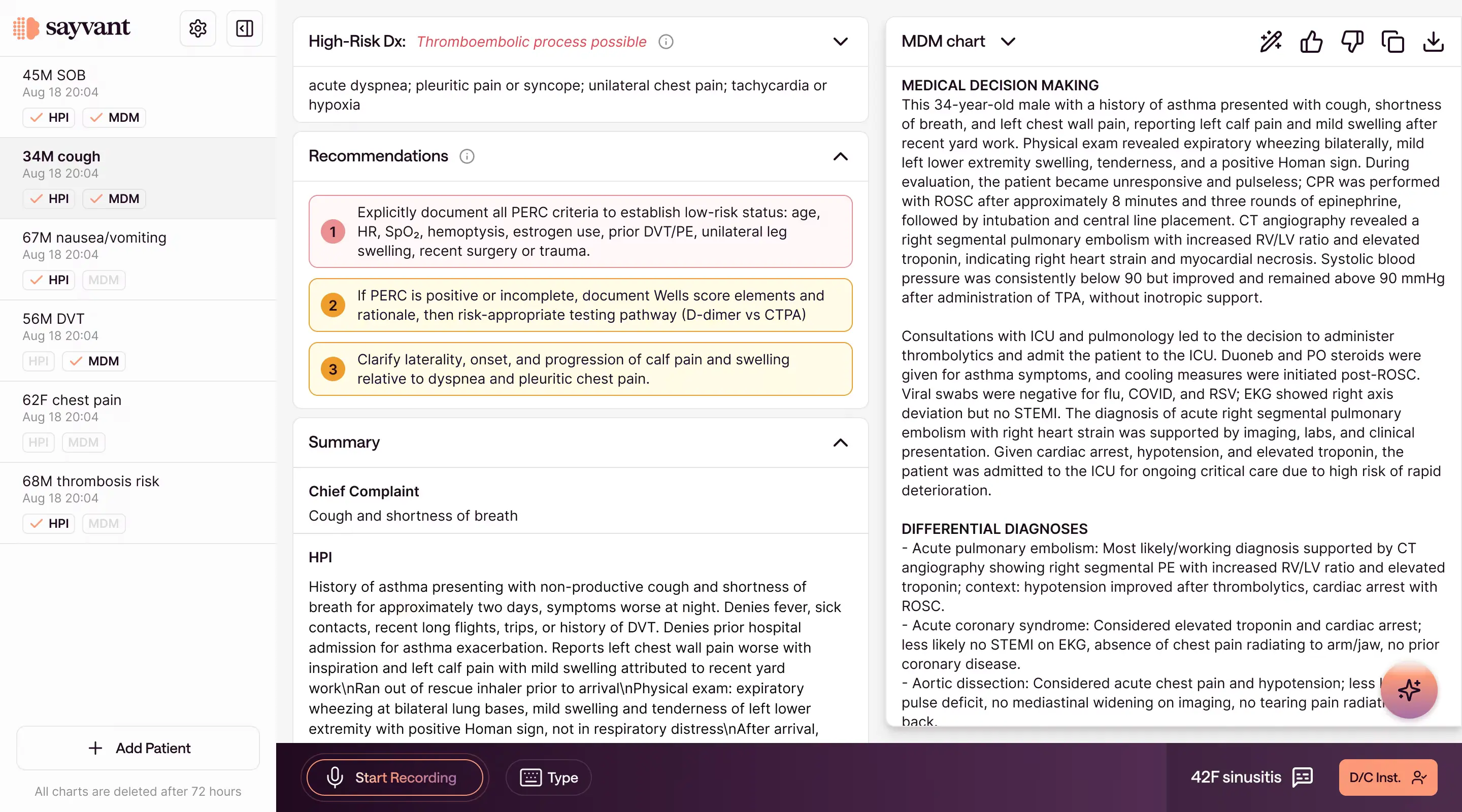
Sayvant generates notes that reflect the clinician's actual reasoning and the complexity of the visit, across the whole stay from ED through discharge.
- Assembles the clinical picture from ambient listening, dictation, and EMR data
- Surfaces differentials and workups for high risk chief complaints
- Drafts full EM and HM notes
Notes are done on shift and the oncoming physician has a full clinical picture.
Held to evidence-based standards
How do you characterize the elevated troponin T — acute myocardial injury, a Type 2 (demand) NSTEMI, or a chronic elevation?
Troponin T: 109.0 ng/L (HH)
Troponin T: 85.5 ng/L (H)
Borderline ST depression, lateral leads
Cardiovascular: RRR. No m/r/g.
Indication: Chest pain.
Impression: No acute cardiopulmonary process.
Reclassify to Type 2 NSTEMI only if serial troponins show a rise/fall with ischemic features; otherwise document acute (non-ischemic) myocardial injury.
Per 4th Universal Definition, document whether serial troponins show a rise/fall with ≥1 ischemic feature (Type 2 MI) or non-ischemic acute myocardial injury; characterize the elevation to code to acuity.
Sayvant checks each diagnosis and plan against clinical evidence and guidelines, and flags potential gaps.
- Surfaces best practices from trusted sources like CMS, ACEP, and BMJ
- Flags missing pertinent information, from re-evaluation time stamps to lab and imaging interpretations
- Reviews medical necessity and clinical appropriateness at admission
Notes withstand quality reviews with improved adherence to desired measures.
Valued for the care delivered
Inpatient admission is supported.
- Bacteremia on blood cultures
- Temperature <35°C or severe immunocompromise
This encounter may qualify for critical care based on sepsis without shock — altered mental status, persistent hypotension with SBP in the low 90s, multiple IV fluid boluses, and treatment with ≥2 IV antibiotics — with ICU admission.
Sayvant documents the care delivered in line with reimbursement guidelines: medical necessity, diagnosis specificity, and complexity of care.
- Validates medical necessity against level of admission criteria
- Identifies diagnosis specificity, linkage, and defensibility gaps impacting DRG capture
- Captures professional fee CPTs, including E/M level and critical care
Charts reflect the true complexity of care delivered, reducing downstream queries, rework, and denials.

The only real-time documentation quality scoring system built for acute care.
SQS is a physician‑validated scoring system, trained by 100s of board‑certified emergency and hospital medicine physicians who actively practice.
Every note is scored for completeness, clinical quality, and financial defensibility. Clinical leaders can quantify incidence, size, and cost of documentation variability across their groups.
Learn more →Higher quality documentation produces measurable results.
Results from a multicenter analysis of 250,000+ encounters across 50 emergency departments and a published survey of Sayvant end users.
From the clinicians who use Sayvanton every shift.